Female Sexual Dysfunction (FSD) is a medical term used for sexual issues, such as weak or no orgasm, Low Libido, and pain during intercourse. When compared with sexual issues in men, FSD is more complicated and less understood. Additionally, research suggests that Sexual Dysfunction (SD) is more common in women than men, with 40% of females and 30% of males experiencing one or more sexual issues.
FSD usually develops due to a combination of factors, such as stress, hormonal changes, relationship issues, or underlying health conditions like Diabetes and ovarian cysts. Effective treatment depends on identifying the specific type of dysfunction, such as pain-related or arousal-related FSD. Once the type is identified, treatment can include FDA-approved medications such as Flibanserin, along with behavioral or physical therapies.
In this article, we will discuss FSD and its symptoms, the female sexual response cycle, and its types. Moreover, you’ll learn the causes of SD in women, diagnostic methods, and effective treatment strategies, including lifestyle changes, FDA-approved medications, and psychological counseling.
Female Sexual Dysfunction and its symptoms
Female Sexual Dysfunction refers to difficulties that prevent a woman from indulging in sexual activities as per her desires. It is a complex condition influenced by physical, psychological, and social factors. Research has indicated that women in their reproductive age are at higher risk of FSD due to various factors like hormonal issues and medication intake. The symptoms of FSD can be:
- Little to no interest in participating in sexual activities (Low Libido).
- Absence of sexual fantasies and thoughts.
- Difficulty becoming or staying aroused, even in the presence of sexual desire.
- Inability or consistent issues in achieving orgasm.
- Experiencing pain (Dyspareunia) and discomfort during vaginal penetration or sexual stimulation.
- Physical changes, such as decreased genital sensation and vaginal dryness.
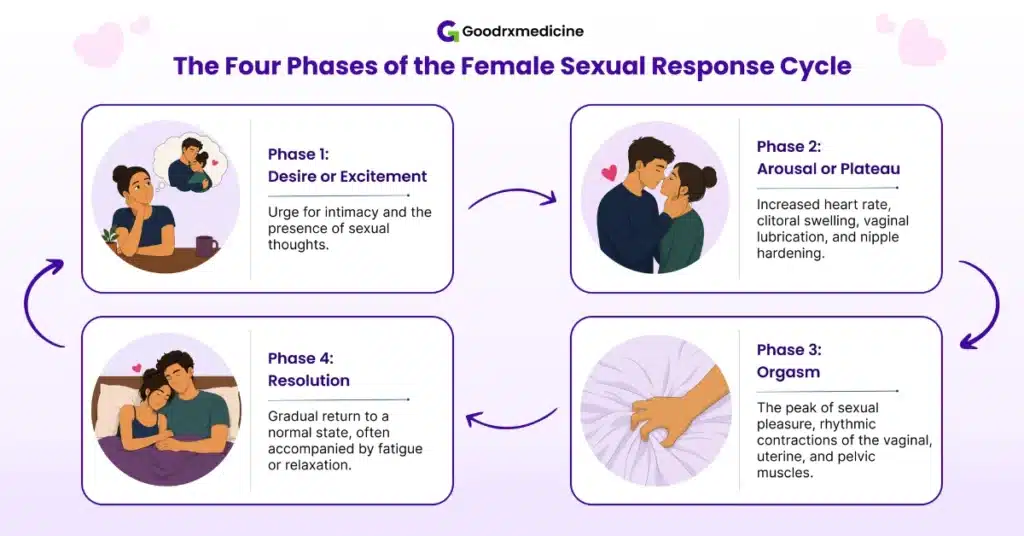
These symptoms can affect different stages of a woman’s sexual response, which include desire, arousal, orgasm, and resolution. Therefore, understanding the normal response cycle can help identify the type of FSD, whether it involves desire, arousal, or another phase.
Types of Female Sexual Dysfunction
FSD is categorized based on the phase of the sexual response cycle it affects. Understanding the types is crucial since each has its own set of causes, symptoms, and treatment approaches.
Desire and arousal disorders
Arousal disorder is the second most common FSD after desire disorder. Given below are these disorders in detail:
- Desire disorder: Low or absent interest in sexual activity that causes distress is known as Hypoactive Sexual Desire Disorder (HSDD).
- Arousal disorder: Difficulty becoming or staying mentally or physically aroused during sexual activity is called Female Sexual Arousal Disorder (FSAD). Arousal disorders can involve reduced genital response, reduced mental excitement, or both.
Earlier, FSAD and HSDD were considered separate disorders. Later, DSM-5 combined them into Female Sexual Interest/Arousal Disorder (FSIAD) since many women experience low arousal and low desire together.
Orgasmic disorders
It is a type of Sexual Dysfunction where there is a constant delay or absence of orgasm, known as Anorgasmia, despite sufficient arousal and stimulation. It is further categorized by:
- Onset: One is lifelong (primary), where a woman has never experienced orgasm under any circumstances. Second is acquired (secondary), where orgasmic function was previously normal but later became infrequent, delayed, or completely absent.
- Situational pattern: It includes Generalized Anorgasmia, where orgasm doesn’t occur with any partner or any form of stimulation, including oral sex, intercourse, masturbation, or sex toys. Another is Situational Anorgasmia, where orgasm happens only in specific situations, like during masturbation but not penetration, or with one partner but not another.
Sexual pain disorders
These disorders, often grouped under a broader term Genito-Pelvic Pain/Penetration Disorder (GPPPD), involve physical pain during or even after sexual activity. Clinical data suggests that approximately 75% females experience pain during sexual intimacy at some point in their lives.
- Dyspareunia: Persistent or recurrent genital pain linked with intercourse.
- Vaginismus: In this, the vaginal opening muscles spasms involuntarily, making it painful or difficult for penetration.
- Vulvodynia: Chronic discomfort, pain, stinging, or burning of the vulva that lasts for 3 months without an identifiable cause.
Save up to 90% on your medicine bills

Lovegra Oral Jelly Rx 100 Mg

Lovegra 100 mg
Starting at just $2.19 per tabletBuy Now
Oestrogel Gel 80 gm
Starting at just $38.02 per tubeBuy Now
Progynova 1 mg
Starting at just $0.20 per tabletBuy NowCauses of Sexual Dysfunction in females
Female Sexual Dysfunction is usually linked to more than one underlying factor. Physical health issues, hormonal shifts, mental well-being, and relationship problems can all contribute, affecting arousal or desire, or causing pain.
Physical Causes
Medical conditions, as well as certain medications, can adversely affect sexual response by causing genital pain or disrupting orgasm. Listed below are these causes in detail:
- Medical conditions: Conditions like Cancer, Diabetes, severe heart disease, kidney impairment, and Multiple Sclerosis (MS) can damage nerve sensation and blood circulation. These two functions are crucial for a healthy sexual life. Moreover, Endometriosis, Pelvic Inflammatory Disease (PID), and ovarian cysts can lead to Dyspareunia.
- Medications: Certain medicines, including antidepressants like Selective Serotonin Reuptake Inhibitors (SSRIs), hormonal contraceptives, blood pressure pills, Cancer medicines, and antihistamines, can cause Low Libido and orgasm difficulties.
Hormonal changes
A significant fluctuation in hormonal levels is observed during specific periods of a woman’s sexual life. This fluctuation can directly influence the desire to get intimate, vaginal lubrication, and overall vaginal health.
- Menopause and perimenopause: During menopause (when periods stop permanently) and perimenopause (transitional phase before menopause), estrogen levels start to fluctuate and drop. In turn, this leads to drying and thinning of vaginal tissues, a condition known as Vaginal Atrophy. It can reduce natural lubrication and make intercourse uncomfortable.
- Postpartum and breastfeeding: After childbirth (postpartum), particularly during breastfeeding, prolactin levels (a hormone involved in milk production) rise. Meanwhile, estrogen levels decrease, resulting in Low Libido and Vaginal Atrophy.
Psychological factors
Sexual response is highly influenced by mental well-being, relationship quality, and mood. Therefore, when these factors are affected, they can interfere with orgasm, desire, and overall sexual satisfaction:
- Mental issues: Depression, Anxiety, and stress can increase cortisol levels (a stress hormone) and keep the body in a fight or flight state. As a result, it lowers sex drive and makes it difficult to get aroused. On the other hand, body image concerns, low self-esteem, and past trauma can make women feel less safe or comfortable, reducing sexual desire.
- Relationship and partner-related factors: Emotional distance, unresolved conflict, or poor communication can reduce sexual interest and satisfaction by lowering emotional safety and making you feel unsupported in the relationship.
- Social and cultural influences: Strict cultural or religious beliefs can create shame, guilt, or Anxiety around sexual activity, which affects arousal, comfort, and orgasm.
Diagnosis of FSD
To be medically diagnosed for FSD, symptoms must persist for at least 6 months and cause significant distress in personal life. The diagnosis of FSD involves the following:
- Medical and sexual history: Your doctor will discuss your symptoms, menstrual cycle status, current medications, past sexual experiences, and mental health issues.
- Screening tools: Questionnaires, such as the Decreased Sexual Desire Screener (DSDS) or the Female Sexual Function Index (FSFI), are used by doctors to assess pain, arousal, and desire.
- Physical examination: Doctors check for physical changes, such as scarring or thinning of genital tissues. They also perform a pelvic examination to assess genital sensitivity and any structural abnormalities or infection.
- Laboratory tests: These include hormonal and blood tests, performed only when clinically indicated to check for underlying conditions, such as Diabetes.
Treatment options for FSD
FSD can be treated by addressing its physical, hormonal, and psychological factors. Moreover, the treatment approach is selected based on severity and body tolerability. Given below are the most common treatment strategies:
Medical treatment
From FDA-approved medications targeting desire disorders to hormonal therapies and emerging interventional options, medical treatment offers the following:
- Estrogen therapy: This therapy restores estrogen levels by directly providing estradiol to improve vaginal sensitivity and dryness. It is available as creams, suppositories, rings, gels, pills (like Progynova 2 mg), and patches. The doctor will decide the most suitable form and dose for you.
- Flibanserin (Addyi): Flibanserin is the first FDA-approved pill for HSDD in both pre- and post-menopausal females. It helps restore sexual desire by increasing dopamine (a feel-good hormone) and reducing serotonin levels (a mood, stress, and sleep regulator) in the body. Generally, a 100 mg tablet is administered at bedtime for around 8 weeks.
- Bremelanotide (Vyleesi): Another FDA-approved HSDD medication for premenopausal women. It is a self-injectable medicine that is usually taken as needed, approximately 45 minutes before planned intercourse.
- Low-intensity shockwave therapy (LiSWT): It is an emerging, painless and non-invasive treatment that delivers acoustic waves to clitoral and vaginal tissue to promote tissue repair and improve blood flow. A 2023 study indicates that it can improve pain and orgasm-related issues.
- Other hormonal treatment: FDA-approved Ospemifene and Prasterone are used for treating Dyspareunia in postmenopausal and menopausal women by functioning like estrogen. Osphena 60 mg is taken as an oral tablet once daily, while Intrarosa 6.5 mg is used as a vaginal insert at bedtime. Both improve lubrication and comfort during intercourse.
Counseling and physical therapy
Behavioral and physical therapies address the psychological, relational, and muscular factors that can’t be managed with hormonal therapy or oral pills. These include:
- Cognitive Behavioral Therapy (CBT): It is the most researched therapy where a therapist reframes negative thoughts around intimacy and body image during counseling to treat orgasmic and arousal difficulties.
- Sex therapy or couples therapy: Sex therapists conduct these to improve relationship communication and use sensate focus to teach enjoying intimacy without performance pressure.
- Pelvic floor physiotherapy: It is considered first-line treatment for GPPPD that releases pelvic floor tension and controls involuntary pelvic floor spasms to enable a pain-free sexual activity.
Lifestyle modifications
Simple but consistent modification to daily habits can significantly improve sexual arousal and desire, especially when FSD is linked with poor cardiovascular health, vaginal discomfort, stress, and imbalanced hormones.
- OTC products: Using OTC lubricants before intercourse can help treat vaginal dryness by reducing discomfort and friction. Vaginal moisturizers are also a preferred option for maintaining vaginal tissue hydration.
- Exercise: 15-30 minutes of regular exercise, like jogging or swimming, can improve cardiovascular health, boost mood, increase libido, and enhance stamina.
- Managing stress: Techniques such as yoga, deep breathing, and mindfulness can control Anxiety and stress, and improve arousal and desire for intimacy.
- Quality sleep: Having 7-9 hours of quality sleep reduces cortisol levels and keeps hormones regulated, which are crucial for sex drive.
- Habits to avoid: Avoid smoking and excessive alcohol intake, as smoking impairs nerve signaling and blood flow. Excessive alcohol is linked with an increased risk of FSD as it disrupts hormonal balance and reduces natural lubrication.
- Diet: Healthy food helps maintain stable nerve and blood vessel function. Some studies have indicated that maintaining a healthy diet, particularly adopting the Mediterranean Diet (MD), can improve SD.
When to see a doctor
While occasional fluctuations in arousal or desire are normal, persistent difficulties that cause significant distress and reduce quality of life require medical attention. Consider seeking a doctor if:
- Sexual difficulties have persisted for 3 to 6 months.
- Symptoms are creating severe personal distress, Anxiety, and an adverse impact on self-esteem.
- Worsening or recurring pain during and/or after intercourse.
- Symptoms of menopause, like vaginal dryness, are interfering with intimacy.
- Lifestyle changes, stress-reduction techniques, and communication with the partner are not providing significant improvement.
Conclusion
Female Sexual Dysfunction is a highly common condition that is characterized by symptoms like low sexual desire, Dyspareunia, vaginal dryness, and reduced genital sensation. The condition affects one or more phases of the sexual response cycle, including sexual desire, arousal, and orgasm.
Furthermore, FSD types include HSDD and FSAD, which are now combined into FSIAD because they often co-occur. Other types are Anorgasmia and pain disorders like Dyspareunia and Vaginismus. SD is mostly caused by factors such as underlying health conditions, like Cancer, antidepressants, hormonal fluctuations during menopause, and psychological issues like Depression and relationship conflicts.
FSD is diagnosed using screening tools such as DSDS and physical examination. After that, doctors recommend treatment like FDA-approved pills, estrogen therapy, or LiSWT. Behavioral and physical therapies also treat FSD by addressing psychological and muscular issues. Additionally, lifestyle changes like a healthy diet and regular exercise also help in the long term. Consult a doctor if sexual issues persist for 3-6 months and significantly interfere with intimacy.

Frequently Asked Questions
How common is Female Sexual Dysfunction?
Female Sexual Dysfunction is highly common, impacting impacts 35.4% to 62.1% women globally. Meanwhile, studies indicate that in the US, it affects around 1 in 5 women aged 18 to 59. Out of this, only 20% of women seek medical consultation.
What is a natural lubricant for female dryness?
Natural lubricants for female dryness include aloe vera gel, organic coconut oil, and vitamin E oil. These lubricants can reduce dryness while reducing friction. However, choose a product without any harsh chemicals and consult a healthcare professional first.
How do I know if I have Sexual Dysfunction as a woman?
You have Sexual Dysfunction as a woman if symptoms like little or no interest in sexual activities, dryness or pain during intercourse, and difficulty reaching orgasm persist for 3 to 6 months and significantly affect your relationship. In this case, it is advised to consult a doctor or a sexual-health specialist.
What medication is used to help a woman climax?
There are no FDA-approved medications specifically to help women achieve orgasm. However, Addyi and Vyleesi can support climax indirectly by improving low sexual desire and arousal. Sildenafil is also sometimes used off-label to improve blood flow, but should only be taken under medical supervision.
GoodRxMedicine only refers to credible, authoritative sources for our content. If you're curious about how we ensure the integrity of our content, we encourage you to read our Content Information Policy.
Julian Carter is a highly accomplished MBA graduate in Pharmaceutical Management, celebrated for his extensive experience and exceptional skills in the pharmaceutical industry. With a wealth of knowledge and expertise, Julian is a valuable contributor to the field and a trusted voice in pharmaceutical management.
As a contributing writer for Goodrxmedicine.com, Julian is committed to educating and empowering individuals to make informed decisions about their health. His passion for the industry is evident in his work, and his dedication to improving the lives of others through education and empowerment is truly remarkable.
With a reputation for excellence and a track record of success, Julian Carter is a respected and admired figure in pharmaceutical management. His insights and contributions to the field are highly valued, and her expertise has helped shape the direction of the industry for the better.
Through his work as a contributing writer for Goodrxmedicine.com and beyond, Julian continues to make a meaningful impact in the lives of many. His commitment to excellence and dedication to improving the health of individuals and communities around the world make him an inspiration to others in the field.